Programmable repair starts at the epithelial surface
OUR MODEL
Find a repair setting with a measurable signal
Quantify TEP and ion-flux changes where epithelial closure can be read objectively.Modulate the signal without hardware
Use topical candidates to adjust endogenous ion transport during the repair window.Advance only on evidence
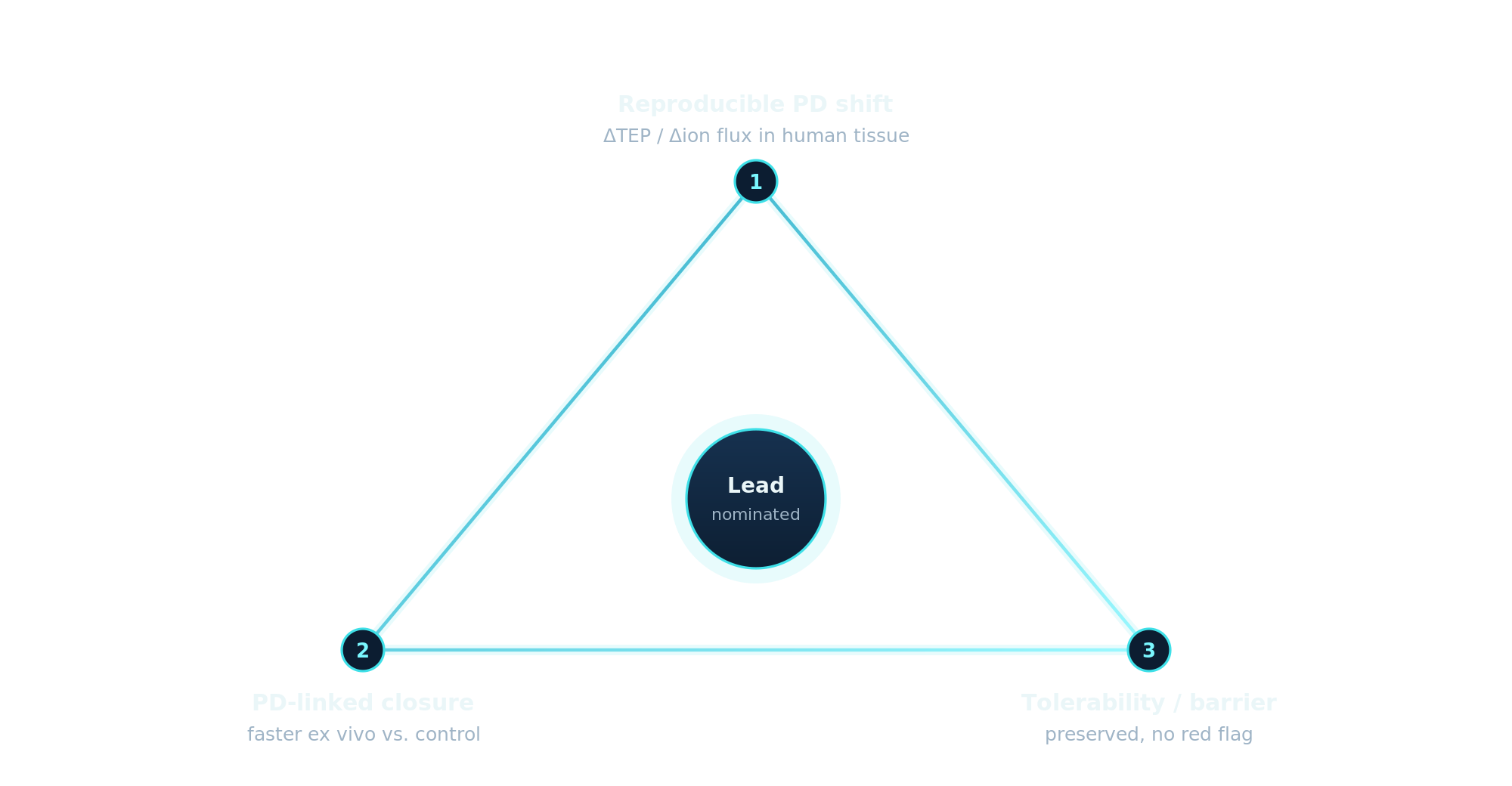
A lead must shift PD, improve closure ex vivo, and reproduce the effect in vivo before additional spend.
Galvanis develops topical therapies that tune endogenous bioelectric signals in impaired ocular surface healing.
The first application is persistent corneal epithelial defects, where closure is visible, time-to-signal is short, and unresolved defects can push patients toward procedural care.
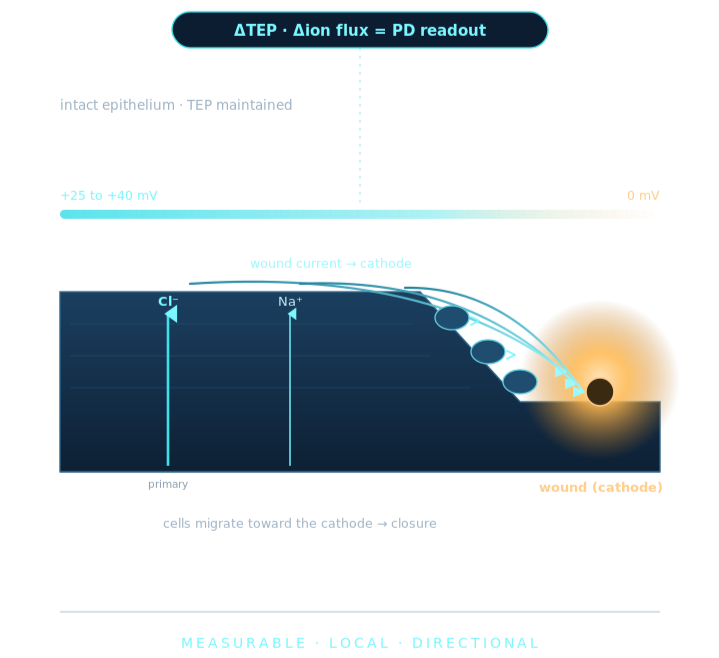
The repair signal can be measured
Epithelial tissues maintain voltage gradients and directional ion flux. When the corneal surface is injured, the circuit is locally interrupted; the surrounding epithelium drives current and electric fields toward the defect.
GALVANIS reads the wound's own electrical signal as a pharmacodynamic marker. The question isn't whether bioelectric repair exists; it's whether a topical candidate can move that signal and shorten closure time in the same model.
Run repair biology like a gated development system
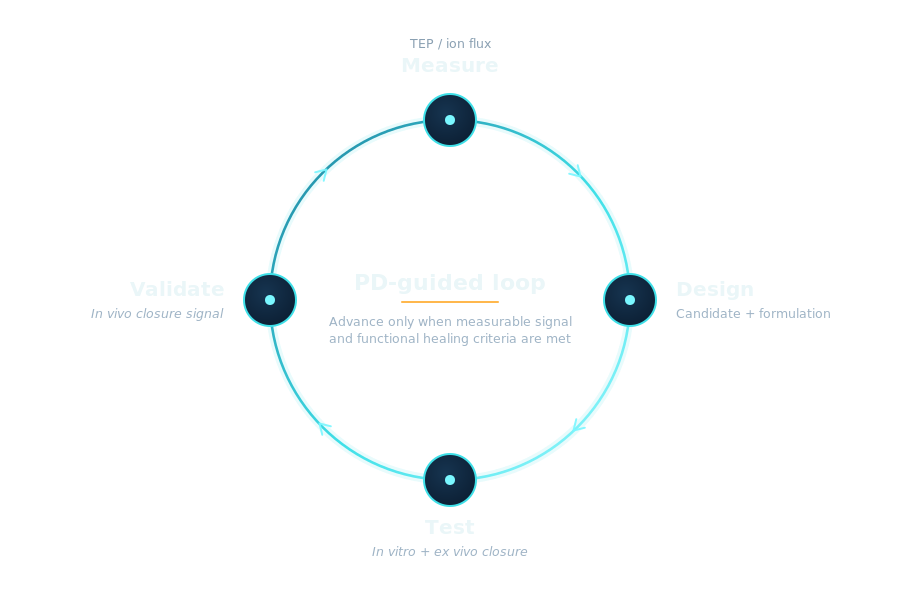
We do not advance a molecule because it looks active in a single closure assay. We advance when a candidate produces a measurable PD shift and that shift travels with functional closure across models.
Start where the biology can be read cleanly
PCED is the beachhead because the defect is visible, closure is objective, topical dosing is local, and failed closure can escalate quickly.
Objective endpoint
Closure can be measured directly with standard ocular-surface imaging.High unmet need
Persistent defects are serious and hard to manage when conventional care fails. PCED is orphan-sized (~100,000/year, U.S.), which supports Orphan Drug economics.Local delivery
The corneal surface supports high local exposure with limited systemic burden.Rapid translational loop
In vitro, ex vivo, and in vivo models can connect PD to closure before a large clinical program.
Focused wedge to repair franchise
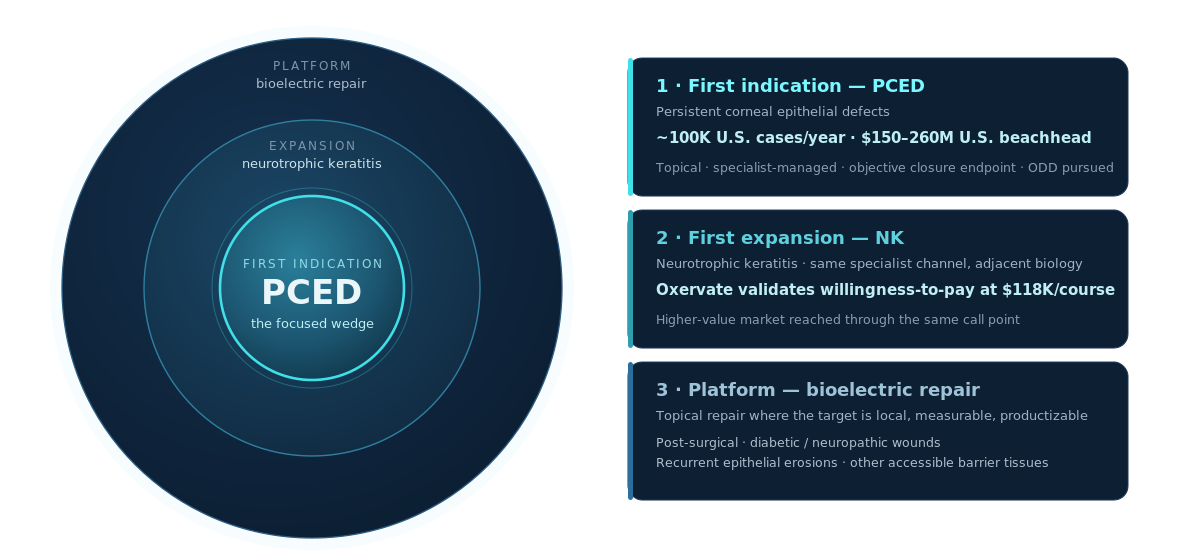
Prove the PD-to-closure link in PCED, then apply the same assay logic to adjacent impaired-healing ocular surface settings.

How we decide what earns the next dollar
A candidate earns the next dollar only by clearing pre-specified PD, closure, and tolerability gates.
North star metrics: one product hypothesis, three gates
2026 focus.
Raise a $2.5M SAFE (~12-month runway) in two milestone-gated tranches, $525K at close, $1.975M at the PD gate, to:
Nominate a PD-validated lead, or stop with discipline
Generate in vivo proof-of-concept
File foundational IP and reach a seed-ready diligence package
Align with the vision
If you’re an investor or clinical partner who believes in regenerative medicine, we should talk.